



Bladder removal
Laparoscopic Radical Cystectomy
The primary treatment for muscle-invasive bladder cancer is the surgical removal of the bladder.
Reasons for which complete bladder removal may be recommended:
• Presence of a muscle-invasive tumor
• Presence of a tumor that grows aggressively, has multiple malignant foci (multifocal), or is superficial but has recurrences after chemotherapy or immunotherapy
• Presence of persistent pain and bleeding in patients with incurable disease.
Bladder removal includes the removal of the bladder, the lower part of the ureters, and pelvic lymph nodes. Depending on factors such as the location of the tumor and the method of urine diversion, part of the adjacent reproductive organs (prostate and seminal vesicles in men, the entire urethra, uterus in women) may also be removed.
Urine Diversion: incontinence or retention.
It is important to understand the two-step approach to bladder removal. First, the bladder and lymph nodes are removed. Then, urine needs to be diverted. This can be achieved in several ways. Generally, we distinguish between options that involve incontinence (continuous flow of urine immediately exiting the body) and retention (urine is stored in the body and diverted as needed). Biological age, kidney function, and other diseases, as well as the patient’s quality of life, are crucial in choosing the surgical strategy.
Ureteral Diversion to the Skin.
Ureteral diversion through the skin (ureterocutaneostomy).
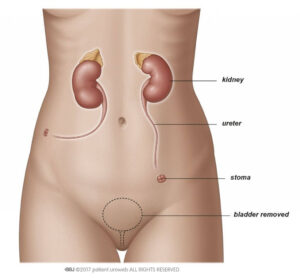
By moving the ureters either together or separately through the skin on the side of the abdomen for urine diversion from the kidneys (stoma) (Fig. 1), urine can simply drain through the stoma into a bag. This method of urine diversion is the simplest. However, it is rarely used. This method is safe and accessible for patients with a complicated medical history (previous surgeries, multiple health issues, palliative care) or for patients who cannot care for themselves after surgery. Major complications are rare; however, recurrent infections and stoma narrowing (stenosis) are common and may require treatment. Patients often need ureteral stenting, which must be changed regularly.
Fig. 1 Ureterocutaneostomy
Placement of a Segment of Small Intestine between the Ureters and Skin: Bricker Procedure (Ileoconduit).

An ileoconduit can be created by placing a segment of small intestine between the ureters and the skin (Fig. 2). This «intestinal stoma» creates a greater distance between the kidneys and the skin and reduces the risk of infection.
Another advantage for patients is that this stoma is easier to manage and has fewer complications, such as narrowing of the outlet (stenosis). This procedure is technically relatively simple and reliable, making it the most commonly used.
Fig. 2 Bricker Procedure.
When choosing this type of urine diversion, you should know that getting used to life with a stoma takes a lot of time and effort.
Formation of a Bladder from Small Intestine: Studer Procedure
A new bladder can be formed from a segment of small intestine that is isolated from the digestive tract (Fig. 3). The reservoir is formed from the small intestine and placed in the pelvis as a replacement for the bladder. Depending on the technique used, the reservoir can have a spherical shape, «W,» «U,» or «V.» The ureters are attached on both sides, and the lower end is connected to the urethra. The urinary sphincter is preserved. In this type of surgery, urine must accumulate and then be expelled as it would with a healthy bladder.
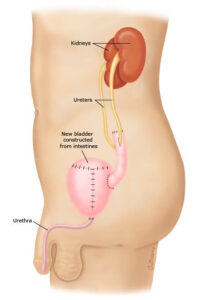
Fig. 3 Bladder from Small Intestine (Studer Procedure)
You will not feel the filling of the bladder or the urge to urinate with a bladder made from small intestine, so emptying must be done every 2-4 hours. The bladder is emptied by relaxing the pelvic floor muscles and contracting the abdominal cavity (Valsalva maneuver). Pressing on the abdomen with both hands can help achieve complete emptying. In 20% of women, periodic self-catheterization is necessary for complete emptying; this is not required for men.
This type of surgery requires satisfactory kidney and liver function, as well as normal pelvic floor muscle condition. Complications after this intervention include recurrent infections (including inflammation of the abdominal wall and kidneys) and urinary incontinence.